Penicillin Allergy
Key messages
- Over-reporting of penicillin allergy leads to unnecessary use of broad-spectrum/less effective alternatives which increases costs, resistance and adverse outcomes such as increased rates of clostridium difficile (CDI), staphylococcus aureus bacteraemia (SAB), longer hospital stays and surgical site infections
- It is important to differentiate between true penicillin allergy and intolerance/side effects. A limited penicillin allergy de-labelling service for in-patients is available at QEUH (contact the ID registrar on-call). For further information on de-labelling, refer to Scottish Antimicrobial Prescribing Group (SAPG) website.
- True penicillin allergy includes Type I reactions (e.g. anaphylaxis, urticaria or rash immediately after penicillin administration) AND Type 4 reactions (e.g. Stevens-Johnson syndrome, DRESS). In cases of intolerance to penicillin (e.g. GI upset) or a minor rash/rash occurring >72 hours after administration, penicillins/related antibiotics should not be withheld unnecessarily in severe infection but the patient must be monitored closely after administration.
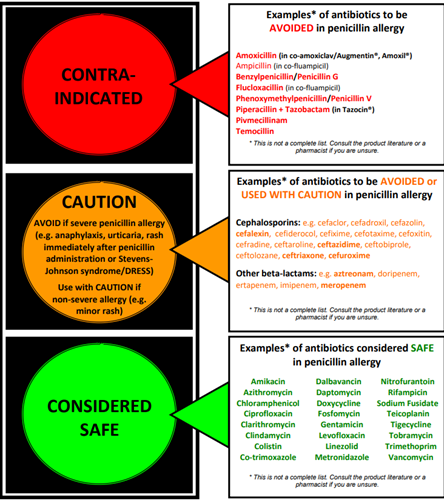
- In true penicillin allergy avoid all penicillins, cephalosporins and other beta-lactam antibiotics (see image below)
- Communicate and document any changes to allergy status across care sectors
- Refer to NHSGGC Penicillin Allergy (Adult) guideline for further information
Published 28/02/2022. Medicines Update blogs are correct at the time of publication.